The five most recognizable signs of a disc bulge are localized back or neck pain that worsens with movement, radiating pain down an arm or leg, numbness or tingling in the extremities, muscle weakness in the affected area, and stiffness that limits your range of motion. These symptoms can appear gradually or strike suddenly after bending, lifting, or even just sitting too long in a poorly supported chair. A person might wake up one morning with a dull ache between the shoulder blades that, over the course of a few weeks, progresses into shooting pain down the left arm — and only then realize the problem started in the spine, not the shoulder.
What makes disc bulges particularly relevant for older adults and those navigating cognitive health concerns is the overlap between spinal pain and reduced mobility, which can accelerate physical decline and worsen quality of life in people already managing conditions like dementia. Chronic pain from an undiagnosed disc bulge can disrupt sleep, increase agitation, and reduce a person’s willingness to stay active — all of which compound cognitive decline. This article walks through each of the five warning signs in detail, explains when a disc bulge might be mistaken for something else, and outlines practical steps for getting the right diagnosis and treatment.
Table of Contents
- What Are the Early Warning Signs of Disc Bulges and How Do They Start?
- Radiating Pain — Why a Disc Bulge Doesn’t Always Hurt Where You Expect
- Numbness, Tingling, and the Nerve Compression Connection
- Muscle Weakness — When to Take Action and What Treatment Options Exist
- Stiffness and Reduced Mobility — The Subtle Sign That Gets Dismissed
- How Disc Bulges Affect Sleep and Cognitive Function in Older Adults
- Advances in Diagnosis and What the Future Holds for Disc Bulge Treatment
- Conclusion
- Frequently Asked Questions
What Are the Early Warning Signs of Disc Bulges and How Do They Start?
A disc bulge occurs when one of the soft, cushion-like discs between the vertebrae pushes outward beyond its normal boundary, often pressing against nearby nerves. The earliest sign is usually a persistent, dull ache in the lower back or neck that doesn’t resolve with rest the way a simple muscle strain would. Unlike a pulled muscle, which tends to improve steadily over a few days, disc-related pain often lingers, shifts in intensity depending on posture, and may feel worse in the morning after a night of lying still. For example, someone who notices that sitting in a car for more than twenty minutes consistently triggers a deep ache in the lower back — but standing and walking relieves it — is describing a pattern more consistent with disc involvement than muscular fatigue.
The reason these early signals get overlooked is that they mimic so many other common complaints. Stiffness after gardening, soreness after a long flight, or an ache that comes and goes over weeks can all feel unremarkable. But a disc bulge doesn’t heal the way soft tissue does. The disc doesn’t have a robust blood supply, so inflammation and mechanical pressure persist longer. What separates a disc bulge from ordinary back pain is the pattern: the pain is positional, it returns predictably with certain movements, and it doesn’t follow the typical arc of a strain that peaks and then steadily fades.

Radiating Pain — Why a Disc Bulge Doesn’t Always Hurt Where You Expect
The second hallmark sign is pain that travels away from the spine and into an arm or leg. When a bulging disc in the lumbar spine presses on the sciatic nerve, the result is sciatica — a burning, electric, or stabbing pain that shoots from the buttock down the back of the leg, sometimes reaching the foot. In the cervical spine, the same mechanism sends pain from the neck into the shoulder, down the arm, and occasionally into the fingers. This referred pain is often more distressing than the back or neck pain itself, and it’s the symptom that most commonly drives people to seek medical attention. However, radiating pain doesn’t always mean a disc bulge is the cause.
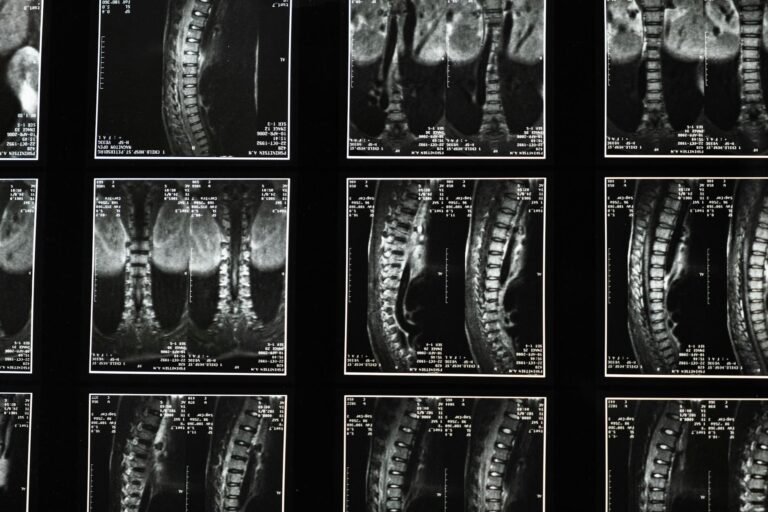
Piriformis syndrome, sacroiliac joint dysfunction, and even peripheral neuropathy from diabetes can produce similar patterns of leg pain. In older adults, spinal stenosis — a narrowing of the spinal canal — can create symptoms nearly identical to a disc bulge. This is why imaging matters. A physical exam can suggest the likely source, but an MRI is typically needed to confirm whether a disc is bulging and, critically, whether it’s actually compressing a nerve. It’s worth noting that many people have disc bulges on imaging that cause no symptoms at all, so the clinical picture and the scan have to match before any treatment decision makes sense.
Numbness, Tingling, and the Nerve Compression Connection
Numbness or tingling — often described as a “pins and needles” sensation — is the third sign and one that tends to alarm people more than pain alone. When a bulging disc compresses a nerve root, it disrupts the normal electrical signals traveling to and from the brain. The result might be a patch of skin on the outer calf that feels numb, a tingling sensation in the thumb and index finger, or a strange buzzing feeling in the bottom of the foot. One common scenario involves a person who notices that their foot keeps “falling asleep” while sitting at a desk, and initially blames the chair, only to discover months later that the problem originates from a disc bulge at the L5-S1 level.
For individuals with dementia or cognitive impairment, this sign is particularly easy to miss. A person who struggles with communication may not be able to articulate that their hand feels numb or that their leg tingles when they walk. Caregivers might notice compensatory behaviors instead — favoring one hand, rubbing a foot repeatedly, or becoming reluctant to grip objects. These behavioral clues are worth paying attention to, especially if they appear alongside other signs on this list. Persistent numbness that lasts more than a few days warrants medical evaluation, because prolonged nerve compression can lead to permanent sensory loss if left untreated.
Muscle Weakness — When to Take Action and What Treatment Options Exist
The fourth sign, muscle weakness, represents a more advanced stage of nerve involvement. When a compressed nerve can no longer send strong signals to the muscles it controls, those muscles begin to lose strength. In the lower body, this might show up as a foot that drags slightly while walking, difficulty rising from a chair, or a knee that buckles unexpectedly. In the upper body, grip strength may decline, or lifting a coffee cup might suddenly feel harder than it should. This weakness is not the same as general fatigue — it’s specific to the muscles supplied by the affected nerve.
The treatment tradeoff at this stage involves deciding between conservative management and surgical intervention. Physical therapy, anti-inflammatory medications, and epidural steroid injections can relieve symptoms for many people and are generally the first line of approach. These conservative treatments work well when the weakness is mild and the nerve compression is moderate. But when muscle weakness is progressive — meaning it’s getting noticeably worse over weeks — or when bowel and bladder function become affected, the calculus shifts toward surgery. A microdiscectomy, which removes the portion of the disc pressing on the nerve, has a high success rate for relieving leg or arm symptoms, but it doesn’t reverse nerve damage that has already become permanent. The window for intervention matters, which is why worsening weakness should never be treated with a wait-and-see approach.
Stiffness and Reduced Mobility — The Subtle Sign That Gets Dismissed
The fifth sign is a gradual loss of flexibility and range of motion in the spine, and it is the one most frequently written off as “just getting older.” A person with a lumbar disc bulge may find that bending forward to tie their shoes has become painful or impossible. Someone with a cervical disc bulge might realize they can no longer turn their head fully to check a blind spot while driving. The stiffness stems from a combination of inflammation around the disc, protective muscle spasms that guard the injured area, and the mechanical obstruction of the bulging disc itself. The limitation here is that stiffness alone is one of the least specific symptoms on this list.
Osteoarthritis, degenerative disc disease without a bulge, and even simple deconditioning can all produce similar restrictions. In older adults who are already less active, the change may be so gradual that it goes unnoticed until a fall or injury forces an evaluation. For people living with dementia, reduced mobility from an undiagnosed disc bulge can be mistakenly attributed entirely to the cognitive condition, leading caregivers and even physicians to overlook a treatable mechanical problem. Any significant change in a person’s willingness or ability to move — especially if it’s asymmetric, affecting one side more than the other — deserves investigation beyond the assumption that it’s just age-related decline.

How Disc Bulges Affect Sleep and Cognitive Function in Older Adults
Chronic pain from a disc bulge disrupts sleep architecture in ways that are particularly damaging for brain health. Deep sleep is when the brain clears metabolic waste products, including beta-amyloid, a protein linked to Alzheimer’s disease. When pain fragments sleep — causing repeated awakenings or preventing the transition into slow-wave sleep — this clearance process is impaired.
A person managing early-stage cognitive decline who also has an untreated disc bulge may experience faster progression of symptoms, not because the disc bulge causes dementia, but because the resulting pain and poor sleep undermine the brain’s recovery mechanisms. In practice, this means that addressing spinal pain in older adults isn’t just an orthopedic concern — it’s a neurological one. A caregiver who notices increased confusion, agitation, or sundowning behaviors in a loved one with dementia should consider whether unmanaged pain might be a contributing factor, particularly if those behavioral changes coincided with reduced mobility or new complaints about the back or neck.
Advances in Diagnosis and What the Future Holds for Disc Bulge Treatment
Diagnostic imaging has improved substantially, with high-resolution MRI now able to distinguish between a disc bulge, a herniation, and other structural abnormalities with much greater precision than even a decade ago. Upright and weight-bearing MRI machines, though still less widely available, can capture the spine under load — revealing bulges that might not appear when a patient is lying flat in a traditional scanner. For older adults who have difficulty lying still for extended periods, faster scan protocols and open MRI designs have made the process more accessible.
On the treatment front, regenerative approaches like platelet-rich plasma injections and intradiscal biologics are being studied, though evidence remains mixed and these therapies are not yet standard of care. What has become clearer over the past several years is that early, targeted physical therapy produces outcomes comparable to surgery for many disc bulges, and that patient education — understanding what movements to avoid, how to maintain spinal stability, and when to escalate care — remains one of the most effective interventions available. The future likely involves better risk stratification, helping clinicians identify earlier which patients will respond to conservative care and which will need surgical intervention before nerve damage becomes irreversible.
Conclusion
The five signs of a disc bulge — localized spinal pain, radiating pain into the limbs, numbness or tingling, muscle weakness, and progressive stiffness — form a recognizable pattern when you know what to look for. Any one of these symptoms in isolation might have an alternative explanation, but when two or more appear together, especially in a pattern that worsens with specific postures or movements, a disc bulge belongs high on the list of possibilities. For older adults and those living with cognitive impairment, these signs are easily masked by other conditions or dismissed as inevitable aging, making vigilant observation by caregivers all the more important.
If you or someone you care for is experiencing these symptoms, the most important next step is a thorough clinical evaluation that includes both a physical exam and, when indicated, imaging. Early intervention — whether through physical therapy, pain management, or surgical referral — can prevent the kind of progressive nerve damage that leads to permanent deficits. Equally important is recognizing that unmanaged spinal pain affects far more than just the back: it disrupts sleep, reduces activity, and can accelerate the very cognitive and physical decline that families are already working hard to slow.
Frequently Asked Questions
Can a disc bulge heal on its own without surgery?
Yes, many disc bulges improve with conservative treatment over six to twelve weeks. The body can reabsorb some of the protruding disc material, and inflammation tends to decrease with time, physical therapy, and appropriate activity modification. Surgery is generally reserved for cases where symptoms are severe, progressive, or unresponsive to conservative care.
How is a disc bulge different from a herniated disc?
A disc bulge involves the disc extending beyond its normal perimeter but remaining intact, somewhat like a hamburger patty that’s wider than its bun. A herniation means the outer layer of the disc has torn and the inner gel-like material has pushed through. Herniations are more likely to compress nerves severely, but bulges can also cause significant symptoms depending on their size and location.
Are disc bulges common in people with dementia?
Disc bulges are common across the aging population regardless of cognitive status. Studies suggest that by age 60, a majority of adults have at least one disc bulge visible on MRI, many of which are asymptomatic. The challenge with dementia patients is not that disc bulges are more frequent, but that the symptoms are harder to identify and communicate.
What is the best sleeping position for a disc bulge?
For lumbar disc bulges, sleeping on the side with a pillow between the knees or on the back with a pillow under the knees tends to reduce pressure on the affected disc. Stomach sleeping generally worsens symptoms because it forces the lumbar spine into extension. For cervical disc bulges, a supportive pillow that maintains the natural curve of the neck is more important than the sleeping position itself.
Can exercise make a disc bulge worse?
It depends on the exercise. High-impact activities, heavy lifting, and movements that involve repeated spinal flexion — like sit-ups or toe touches — can aggravate a disc bulge. However, targeted exercises that strengthen the core and improve spinal stability, often prescribed by a physical therapist, are a cornerstone of treatment and typically reduce symptoms over time.