Dementia kills by progressively destroying brain cells until the damage reaches regions of the brain that control essential bodily functions like breathing, heart rate, and swallowing. It is a terminal neurodegenerative disease, though death rarely comes from the brain damage alone. Instead, the overwhelming majority of dementia patients die from complications that arise because the brain can no longer coordinate the body’s basic survival mechanisms. The most common of these fatal complications are aspiration pneumonia, sepsis, cardiovascular events, and severe malnutrition or dehydration, a condition known as cachexia. Consider a person in the late stages of Alzheimer’s disease who can no longer swallow safely.
Food particles slip past the epiglottis and enter the lungs, seeding an infection. Because dementia has also degraded the immune system’s responsiveness, the body cannot fight off the pneumonia. This is the single most common way Alzheimer’s patients die, and it illustrates the cruel chain reaction that defines end-stage dementia: the brain fails, then the body follows. In the United States, 120,122 deaths from Alzheimer’s were officially recorded in 2022, and deaths from the disease have increased by more than 142 percent since 2000, even as deaths from stroke, heart disease, and HIV have declined. This article explains, in medical terms, how dementia moves through the brain and what happens at each stage, the specific complications that prove fatal, who is most at risk, how long patients typically survive after diagnosis, and what families should understand about the trajectory of this disease.
Table of Contents
- What Happens in the Brain When Dementia Causes Death?
- The Leading Causes of Death in Dementia Patients
- Sepsis, Falls, and the Hidden Dangers of Advanced Dementia
- How Long Do People Live After a Dementia Diagnosis?
- Who Is Most Affected, and Why Death Rates Keep Rising
- The Financial Weight of a Disease That Kills Slowly
- What Research and Policy May Change in the Coming Years
- Conclusion
- Frequently Asked Questions
What Happens in the Brain When Dementia Causes Death?
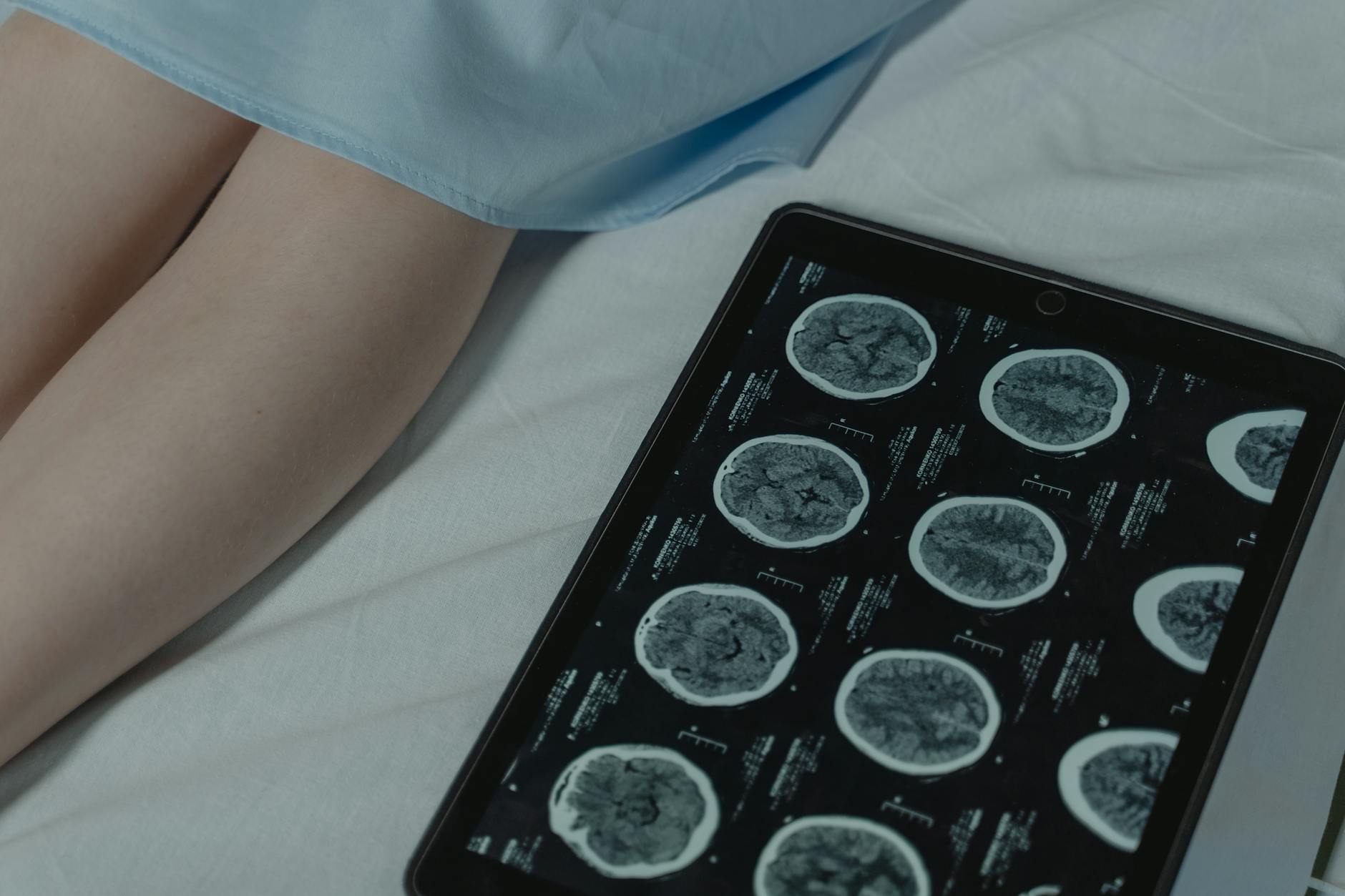
Alzheimer’s disease, the most common form of dementia, typically begins in the hippocampus and entorhinal cortex, the regions responsible for forming new memories. Abnormal proteins, primarily amyloid plaques and tau tangles, accumulate and kill neurons in these areas first. Over months and years, the damage spreads outward to the temporal and frontal lobes, impairing language, judgment, and personality. But the truly fatal progression happens when neurodegeneration reaches the brainstem. The brainstem is the body’s autopilot. It regulates breathing, heart rhythm, blood pressure, and the complex muscular coordination required to swallow food and clear the airway. Once these circuits are compromised, the body loses its ability to perform the functions that keep a person alive. This progression is not metaphorical. Imaging studies show that the brain of a person with advanced Alzheimer’s has dramatically shrunk, with widened grooves on the surface and enlarged ventricles filled with fluid where healthy tissue once existed. The cortex, which handles thinking and planning, thins severely.
But it is the damage to deeper structures that proves lethal. When the brainstem’s respiratory centers falter, breathing becomes irregular and shallow. When the swallowing reflex fails, aspiration becomes nearly inevitable. The person does not die because they forgot their family. They die because their brain can no longer tell their lungs to breathe or their throat to close when food approaches. It is worth noting that not all dementias follow the same anatomical path. Frontotemporal dementia begins in the frontal and temporal lobes, initially causing personality changes and language problems rather than memory loss. Lewy body dementia involves abnormal protein deposits in areas that affect movement, cognition, and autonomic function simultaneously. Vascular dementia results from impaired blood flow to the brain, often from a series of small strokes. Each type damages different regions at different rates, which partly explains why survival times vary so significantly across dementia subtypes.
The Leading Causes of Death in Dementia Patients
Research consistently identifies three primary immediate causes of death in people with dementia: cachexia and dehydration, accounting for roughly 35.2 percent of deaths; cardiovascular disorders at 20.9 percent; and acute pulmonary diseases, predominantly pneumonia, at 20.1 percent. These numbers come from autopsy and clinical studies, and they underscore that dementia patients rarely die from a single cause. Multiple organ systems are failing simultaneously by the end. Aspiration pneumonia deserves particular attention because it is the leading specific cause of death in Alzheimer’s patients. The mechanism is straightforward but devastating. As the brain loses control of the swallowing reflex, food, liquids, or even saliva can be misdirected into the trachea and lungs rather than the esophagus. The foreign material introduces bacteria into the lungs, triggering infection. A meta-analysis published in the medical literature found that the risk of pneumonia-associated death is increased more than twofold in patients with dementia compared to those without. For a healthy older adult, a bout of pneumonia is serious but often survivable with antibiotics and supportive care.
For someone with advanced dementia, the immune system is too compromised and the body too weakened to mount an effective defense. However, it is important to understand that these statistics reflect averages across large populations. Individual cases can look very different. Some patients with dementia die suddenly from a heart attack or stroke, never reaching the stage where swallowing becomes dangerous. Others linger for years in a severely debilitated state. The type of dementia matters as well. Vascular dementia, for instance, carries a higher risk of cardiovascular death because the same blood vessel damage causing the dementia also threatens the heart. Families should be cautious about assuming any single trajectory. The disease is broadly predictable but individually unpredictable.
Sepsis, Falls, and the Hidden Dangers of Advanced Dementia
Beyond pneumonia and malnutrition, several other complications kill dementia patients at alarming rates, often because the warning signs go unrecognized. Sepsis is among the most dangerous. People with advanced dementia are highly vulnerable to infections, particularly urinary tract infections, that go undetected because the patient can no longer communicate symptoms like burning, pain, or fever. A UTI that would prompt a quick doctor visit for a cognitively healthy person can silently escalate to a bloodstream infection. Once sepsis takes hold, organ failure can progress rapidly, and mortality rates are high even with aggressive treatment. Falls represent another major threat that is easy to underestimate. Dementia impairs spatial awareness, balance, and judgment, making falls frequent. A broken hip in an 85-year-old with dementia is not simply an orthopedic problem. Research shows that dementia patients who fall are more likely to develop sepsis and surgical site complications than those without dementia, and they have higher associated death rates.
The surgery itself carries risks of delirium and accelerated cognitive decline, the recovery demands cooperation and physical therapy that a confused patient cannot reliably participate in, and immobility during recovery increases the risk of blood clots and pneumonia. A fall that might be a setback for a healthy older adult can trigger a cascade that proves fatal for someone with dementia. One specific scenario illustrates how these dangers compound. An elderly woman with moderate Alzheimer’s trips on a rug at home and fractures her hip. She is hospitalized and undergoes surgery, but during recovery she becomes agitated and pulls at her IV line. She develops a surgical wound infection that is not caught early because she cannot describe her pain. The infection enters her bloodstream, and she develops sepsis. She dies twelve days after the fall. On the death certificate, the cause of death may be listed as sepsis or surgical complications, but dementia was the underlying driver of every step in that sequence.

How Long Do People Live After a Dementia Diagnosis?
The average life expectancy after a dementia diagnosis is commonly cited as eight to ten years, but this number obscures enormous variation depending on the patient’s age, sex, overall health, and the type of dementia. A woman diagnosed around age 60 may survive approximately 8.9 years, while a man diagnosed around age 85 may live only about 2.2 years. Women survive roughly 1.5 years longer than men at all ages after diagnosis. Dementia reduces overall life expectancy by about 13 years for someone diagnosed at 65, but only by about 2 years for someone diagnosed at 85, largely because older patients have less remaining life expectancy to lose. Survival also varies considerably by dementia type. Alzheimer’s disease, with its relatively slow progression, has a typical survival range of 8 to 12 years. Vascular dementia is more aggressive, with an average survival of about 4 years, partly because the cardiovascular problems causing it also threaten other organs. Lewy body dementia falls in the middle at 5 to 7 years, though the range can stretch from 2 to 20 years in outlier cases.
Frontotemporal dementia averages about 8 years. These are statistical averages, and individual cases can diverge widely. A person diagnosed with Alzheimer’s at 62 who is otherwise physically healthy and receives strong care may live 15 years. Another person diagnosed at 78 with multiple comorbidities may decline rapidly over 3 years. The tradeoff families face when interpreting these numbers is between hope and preparation. Knowing that the average is 8 to 10 years might encourage early financial and legal planning, but it can also create a false sense of time. Some patients decline far faster than expected, particularly if they develop pneumonia or sepsis early. Others plateau for long periods before a sudden decline. Clinicians generally advise families to plan for a long course while remaining prepared for rapid changes, particularly once the patient enters the late stage and loses the ability to walk, speak, or swallow safely.
Who Is Most Affected, and Why Death Rates Keep Rising
The demographics of Alzheimer’s disease reveal stark disparities. Almost two-thirds of Americans living with Alzheimer’s are women, a gap that is only partly explained by women’s longer average lifespans. Hormonal changes after menopause, genetic risk factors, and differences in brain structure and connectivity are all being studied as contributing factors. Racial and ethnic disparities are equally significant. Older Black Americans are about twice as likely to have Alzheimer’s as older White Americans, and older Hispanic Americans are about 1.5 times as likely. These disparities are driven by a complex mix of factors including rates of cardiovascular disease, access to healthcare, socioeconomic conditions, and potentially genetic differences in risk. In 2025, an estimated 7.2 million Americans age 65 and older are living with Alzheimer’s, roughly 1 in 9 people over 65.
Without major medical breakthroughs, that number could reach 13.8 million by 2060. Alzheimer’s is currently the 7th leading cause of death in the United States, a ranking that dropped from 6th only because COVID-19 entered the top ten in 2020. Data from 2023 suggest it will likely resume its position as the 6th leading cause. Critically, dementia-related death rates remain higher than pre-pandemic levels even though both COVID-19 and dementia death rates have declined since the 2020 peak. A limitation of all these statistics is that dementia deaths are almost certainly undercounted. When a patient with Alzheimer’s dies of pneumonia, the death certificate may list pneumonia as the cause of death without noting dementia as the underlying condition. Studies comparing clinical records to death certificates consistently find that dementia is underreported as a contributing cause. The true toll of dementia-related mortality is likely significantly higher than official numbers suggest, which means that public health resources and research funding may not yet reflect the actual scale of the crisis.
The Financial Weight of a Disease That Kills Slowly
Dementia’s lethality is compounded by the financial devastation it inflicts on families long before the patient dies. Projected health and long-term care costs for people with Alzheimer’s and other dementias are expected to reach $384 billion in 2025, a figure that excludes unpaid caregiving entirely. When unpaid care is factored in, the picture becomes even more staggering: nearly 12 million Americans provide unpaid dementia care, contributing more than 19 billion hours valued at over $413 billion in 2024. Unlike a heart attack or a cancer diagnosis, which may involve intense but relatively time-limited treatment, dementia requires years of escalating care.
A family member who begins by helping with finances and medication management may eventually be providing round-the-clock personal care, including feeding, bathing, and managing behavioral symptoms. Many caregivers reduce their work hours or leave the workforce entirely, compounding the financial damage. By the time the patient enters the final stage, families have often spent down savings, taken on debt, or placed their loved one in a memory care facility that costs $5,000 to $8,000 per month or more. The disease kills the patient, but it can financially ruin the family.
What Research and Policy May Change in the Coming Years
The approval of anti-amyloid immunotherapies like lecanemab and donanemab in recent years represents the first time treatments have been shown to modestly slow the progression of early-stage Alzheimer’s by targeting the underlying disease biology rather than just managing symptoms. These drugs are not cures. They slow cognitive decline by roughly 25 to 35 percent in clinical trials and carry serious risks including brain swelling and microbleeds. But they represent a proof of concept that the disease can be modified, which has energized research into more effective next-generation therapies targeting tau protein, neuroinflammation, and metabolic dysfunction in the brain.
The more immediate impact for most families, however, will come from improvements in early detection, palliative care, and caregiver support. Blood tests for Alzheimer’s biomarkers are becoming increasingly accurate and accessible, which could allow diagnosis years before symptoms become debilitating. Earlier diagnosis means earlier planning, earlier access to clinical trials, and earlier intervention with whatever treatments are available. On the policy side, the projected growth of the dementia population to nearly 14 million by 2060 will force difficult conversations about Medicare funding, long-term care infrastructure, and the sustainability of relying on unpaid family caregivers. How societies respond to those challenges will shape the experience of dying with dementia as much as any drug.
Conclusion
Dementia causes death through a relentless progression of brain damage that eventually compromises the body’s most basic survival functions. The brain loses its ability to coordinate swallowing, fight infections, regulate the heart, and maintain nutrition. The result is a cascade of complications, primarily aspiration pneumonia, sepsis, cardiovascular failure, and cachexia, that prove fatal in a body too weakened to resist. With more than 120,000 recorded deaths per year in the United States and a 142 percent increase in Alzheimer’s mortality since 2000, the scale of this crisis is immense and growing.
For families navigating a dementia diagnosis, understanding how the disease kills is not morbid. It is practical. It informs decisions about advance directives, palliative care, feeding interventions, and end-of-life planning. It helps caregivers recognize the warning signs of pneumonia or sepsis that might otherwise be missed in a patient who cannot describe their symptoms. And it underscores the urgency of both medical research and policy investment in a disease that currently has no cure and is projected to affect nearly 14 million Americans within a generation.
Frequently Asked Questions
Is dementia itself listed as the cause of death, or is it the complications?
It depends on the certifying physician. In many cases, the immediate cause of death is listed as pneumonia, sepsis, or cardiac arrest, with dementia noted as a contributing or underlying condition. However, data from 2022 show that dementia itself was listed as the underlying cause of death in 64.6 percent of dementia-related deaths in adults 65 and older, with heart disease at 9.1 percent and stroke at 4.6 percent. Reporting practices vary significantly, and many experts believe dementia is still undercounted on death certificates.
How long can someone live after being diagnosed with dementia?
The average is 8 to 10 years, but the range is wide. Survival depends heavily on age at diagnosis, sex, type of dementia, and overall health. Women diagnosed around age 60 may live nearly 9 years, while men diagnosed around age 85 may live just over 2 years. Alzheimer’s tends to have the longest survival at 8 to 12 years, while vascular dementia is shorter at roughly 4 years.
Why is pneumonia so dangerous for people with dementia?
Dementia damages the brain’s ability to coordinate the swallowing reflex, causing food, liquid, or saliva to enter the lungs instead of the stomach. This is called aspiration, and it introduces bacteria that cause pneumonia. Because dementia also weakens the immune system and the patient often cannot communicate symptoms, the infection may not be caught early. The risk of dying from pneumonia is more than doubled in dementia patients compared to those without the disease.
Can dementia be prevented or cured?
There is currently no cure for any form of dementia. New immunotherapy drugs like lecanemab can modestly slow early-stage Alzheimer’s progression but do not stop or reverse the disease. Reducing cardiovascular risk factors, staying physically and mentally active, managing hearing loss, and avoiding excessive alcohol use may lower the risk of developing dementia, but they do not eliminate it. Research is ongoing and accelerating.
Are certain racial or ethnic groups more affected by Alzheimer’s?
Yes. Older Black Americans are about twice as likely to have Alzheimer’s as older White Americans, and older Hispanic Americans are about 1.5 times as likely. These disparities reflect a combination of genetic factors, higher rates of cardiovascular disease, differences in healthcare access, and socioeconomic conditions. Almost two-thirds of all Americans with Alzheimer’s are women.
What does end-stage dementia look like?
In the final stage, patients typically lose the ability to walk, sit upright, speak, or swallow safely. They may not recognize family members and require total assistance with all daily activities. The most common causes of death at this stage are aspiration pneumonia, infections leading to sepsis, and severe weight loss from the inability to eat and drink. This stage can last from several months to more than two years.





